Obstruted Defaecation Web
| Perineal Procedures for ODS | |||||||||||||||||||||||||||
|
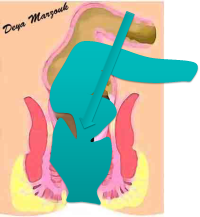
Recognition of ODS as a symptom complex and its relationship to rectal wall abnormalities was follwed by development of operations to treat it, mostly using a perineal approach. This was a natural extension for operations done for rectocoeles and external prolapse. These included (among others):
The published results of Intra-anal Delorme's for Internal rectal prolapse
Comments: As expected the series include only small number of patients, are very heterogenous in terms of patients selection criteria, the actual technique used and the method af assessing improvement in symptoms. There is great divergence in the success rates reported as well. My own experience with this procedure over 15 years explains all of these variations in a way. I initially used this procedure in what I would now classify as type 3 internal rectal prolapse and started noting good results. As I gained operative experience, I started tackling more and more difficult cases and I started noticing that those with higher internal prolapse [type 2], did not necessarily fare as well. I thought that this must be due to the higher point of intussusception and therefore in the more difficult cases, it may be that the operation was not perfect, leaving behind some internal intussusception. So would an improvement in the technique produce better result, e.g. Using a Trans-STARR to get a higher resection inside the rectum. I doubt it, simply, because all transperineal approaches would not tackle other intra-abdominal factors or a bad S shaped rectum. This is immediately understood, once surgeons start using laparoscopy in these patients. I think perineal procedures success rate will hover long term around the 50% mark, not only because of missing intra-abdominal factors in ODS, but also because long term patients with come back with recurrent intussusception above the anastomotic line, clearly evidence of the influence of redundant colon falling down again So what is explanation of the high success rate reported by some of the other authors. It probably reflects both very strict selection of patients suitable for perineal approach as well as short term follow-up Dippolito in his series from 2005, described using anterior Delorme's procedure [limiting the operation to the front half of rectum] in 13 patients, while 14 had full Delorme's procedure. I used Anterior Delorme's in only one patient in 2003, [who had a rectocoele and an internal rectal intussusception], because it was very difficult to do the posterior half and it worked well in controlling the post defaecation leakage. So even half a Delorme's worked, probably because of lucky selection. This again illustrates the point that perineal operations can be effective if they target patients with isolated rectocoele & intussusception and without additional intra-abdominal factors. Even in those with intra-abdominal factors, it is likely that some patients will benefit, but the benefit may not be sustained. |